Abdelrahman, Islam Fathy Soliman, Amr Abdel Raheem, Yaser Elkhiat, Abdelrahman A. Aburahma, Tarek Abdel-Raheem, and Hussein Ghanem. “Safety and Efficacy of Botulinum Neurotoxin in the Treatment of Erectile Dysfunction Refractory to Phosphodiesterase Inhibitors: Results of a Randomized Controlled Trial.” Andrology 10, no. 2 (2022): 254–61. https://doi.org/10.1111/andr.13104.
Ausó, Eva, Violeta Gómez-Vicente, and Gema Esquiva. “Visual Side Effects Linked to Sildenafil Consumption: An Update.” Biomedicines 9, no. 3 (March 12, 2021): 291. https://doi.org/10.3390/biomedicines9030291.
Chung, Eric. “Medical Sciences A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction,” 2019, 1–11.
Costa, Pierre, Gilles Grandmottet, Hien Duc Mai, and Stéphane Droupy. “Impact of a First Treatment with Phosphodiesterase Inhibitors on Men and Partners’ Quality of Sexual Life: Results of a Prospective Study in Primary Care.” The Journal of Sexual Medicine 10, no. 7 (July 2013): 1850–60. https://doi.org/10.1111/jsm.12186.
El-Shaer, Waleed, Hussein Ghanem, Tamer Diab, Ahmed Abo-Taleb, and Wael Kandeel. “Intra-Cavernous Injection of BOTOX® (50 and 100 Units) for Treatment of Vasculogenic Erectile Dysfunction: Randomized Controlled Trial.” Andrology 9, no. 4 (2021): 1166–75. https://doi.org/10.1111/andr.13010.
El‐Shaer, Waleed, Hussein Ghanem, Tamer Diab, Ahmed Abo‐Taleb, and Wael kandeel. “Intra‐cavernous Injection of BOTOX ® (50 and 100 Units) for Treatment of Vasculogenic Erectile Dysfunction: Randomized Controlled Trial.” Andrology 9, no. 4 (July 2021): 1166–75. https://doi.org/10.1111/andr.13010.
Siroky, Mike B., and Kazem M. Azadzoi. “Vasculogenic Erectile Dysfunction: Newer Therapeutic Strategies.” Journal of Urology 170, no. 2S (August 2003): S24–30. https://doi.org/10.1097/01.ju.0000075361.35942.17.
Cayetano‐Alcaraz, Axel Alberto, Tharu Tharakan, Runzhi Chen, Nikolaos Sofikitis, and Suks Minhas. “The Management of Erectile Dysfunction in Men with Diabetes Mellitus Unresponsive to Phosphodiesterase Type 5 Inhibitors.” Andrology 11, no. 2 (February 2023): 257–69. https://doi.org/10.1111/andr.13257.
Geelhoed, Jeannette P., Olivier Wegelin, Ellen Tromp, Bert‐Jan De Boer, Igle‐Jan De Jong, and Jack J. H. Beck. “Improvement in the Ability to Have Sex in Patients with Peyronie’s Disease Treated with Collagenase Clostridium histolyticum .” BJUI Compass 4, no. 1 (January 2023): 66–73. https://doi.org/10.1002/bco2.185.
Lin, Haocheng, and Run Wang. “The Science of Vacuum Erectile Device in Penile Rehabilitation after Radical Prostatectomy.” Translational Andrology and Urology 2, no. 1 (2013).
———. “The Science of Vacuum Erectile Device in Penile Rehabilitation after Radical Prostatectomy.” Translational Andrology and Urology 2, no. 1 (2013).
Welliver, R. Charles, Clay Mechlin, Brianne Goodwin, Joseph P. Alukal, and Andrew R. McCullough. “A Pilot Study to Determine Penile Oxygen Saturation Before and After Vacuum Therapy in Patients with Erectile Dysfunction After Radical Prostatectomy.” The Journal of Sexual Medicine 11, no. 4 (April 1, 2014): 1071–77. https://doi.org/10.1111/jsm.12445.
Culha, Mehmet Gokhan, Erkan Erkan, Tugce Cay, and Uğur Yücetaş. “The Effect of Platelet-Rich Plasma on Peyronie’s Disease in Rat Model.” Urologia Internationalis 102, no. 2 (2019): 218–23. https://doi.org/10.1159/000492755.
Geelhoed, Jeannette P., Olivier Wegelin, Ellen Tromp, Bert‐Jan De Boer, Igle‐Jan De Jong, and Jack J. H. Beck. “Improvement in the Ability to Have Sex in Patients with Peyronie’s Disease Treated with Collagenase Clostridium histolyticum .” BJUI Compass 4, no. 1 (January 2023): 66–73. https://doi.org/10.1002/bco2.185.
“Peyronie’s Disease in a Patient after COVID‐19 Infection_ A Case Report _ Enhanced Reader.” Accessed August 18, 2021. https://doi.org/10.1111/and.14219.
Raheem, Amr Abdel, Giulio Garaffa, Tarek Abdel Raheem, Michelle Dixon, Amanda Kayes, Nim Christopher, and David Ralph. “The Role of Vacuum Pump Therapy to Mechanically Straighten the Penis in Peyronie’s Disease.” BJU International 106, no. 8 (2010): 1178–80. https://doi.org/10.1111/j.1464-410X.2010.09365.x.
Safarinejad, M R. “Safety and Efficacy of Coenzyme Q10 Supplementation in Early Chronic Peyronie’s Disease: A Double-Blind, Placebo-Controlled Randomized Study.” International Journal of Impotence Research 22, no. 5 (2010): 298–309. https://doi.org/10.1038/ijir.2010.20.
Virag, Ronald, Hélène Sussman, Sandrine Lambion, and Valérie de Fourmestraux. “Evaluation of the Benefit of Using a Combination of Autologous Platelet Rich-Plasma and Hyaluronic Acid for the Treatment of Peyronie’s Disease.” Sexual Health Issues 1, no. 1 (2017). https://doi.org/10.15761/SHI.1000102.
Bosma-Den Boer, Margarethe M., Marie Louise Van Wetten, and Leo Pruimboom. “Chronic Inflammatory Diseases Are Stimulated by Current Lifestyle: How Diet, Stress Levels and Medication Prevent Our Body from Recovering.” Nutrition and Metabolism 9 (2012). https://doi.org/10.1186/1743-7075-9-32.
Casabona, Francesco, Ilaria Gambelli, Federica Casabona, Pierluigi Santi, Gregorio Santori, and Ilaria Baldelli. “Autologous Platelet-Rich Plasma (PRP) in Chronic Penile Lichen Sclerosus: The Impact on Tissue Repair and Patient Quality of Life.” International Urology and Nephrology 49, no. 4 (April 2017): 573–80. https://doi.org/10.1007/s11255-017-1523-0.
Chung. “A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction.” Medical Sciences 7, no. 9 (August 29, 2019): 91. https://doi.org/10.3390/medsci7090091.
Chung, Eric. “Medical Sciences A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction,” 2019, 1–11.
Everts, Peter, Kentaro Onishi, Prathap Jayaram, José Fábio Lana, and Kenneth Mautner. “Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020.” International Journal of Molecular Sciences 21, no. 20 (October 21, 2020): 7794. https://doi.org/10.3390/ijms21207794.
Garcia, MM, TM Fandel, G Lin, AW Shindel, L Banie, CS Lin, and TF Lue. “Treatment of Erectile Dysfunction in the Obese Type 2 Diabetic ZDF Rat with Adipose Tissue-Derived Stem Cells,” 2010, 14.
Israeli, Joseph M., Soum D. Lokeshwar, Iakov V. Efimenko, Thomas A. Masterson, and Ranjith Ramasamy. “The Potential of Platelet-Rich Plasma Injections and Stem Cell Therapy for Penile Rejuvenation.” International Journal of Impotence Research, November 6, 2021, 1–8. https://doi.org/10.1038/s41443-021-00482-z.
Kumar, C.S. “265 Combined Treatment of Injecting Platelet Rich Plasma With Vacuum Pump for Penile Enlargement.” The Journal of Sexual Medicine 14, no. 1 (January 2017): S78. https://doi.org/10.1016/j.jsxm.2016.11.174.
Littara, A., B. Palmieri, V. Rottigni, and T. Iannitti. “A Clinical Study to Assess the Effectiveness of a Hyaluronic Acid-Based Procedure for Treatment of Premature Ejaculation.” International Journal of Impotence Research 25, no. 3 (2013). https://doi.org/10.1038/ijir.2013.13.
Liu, Ming-Che, Meng-Lin Chang, Ya-Chun Wang, Wei-Hung Chen, Chien-Chih Wu, and Shauh-Der Yeh. “Revisiting the Regenerative Therapeutic Advances Towards Erectile Dysfunction.” Cells 9, no. 5 (May 19, 2020): 1250. https://doi.org/10.3390/cells9051250.
Masterson, Thomas A., Manuel Molina, Braian Ledesma, Isaac Zucker, Russell Saltzman, Emad Ibrahim, Sunwoo Han, Isildinha M. Reis, and Ranjith Ramasamy. “Platelet-Rich Plasma for the Treatment of Erectile Dysfunction: A Prospective, Randomized, Double-Blind, Placebo-Controlled Clinical Trial.” Journal of Urology, April 30, 2023, 10.1097/JU.0000000000003481. https://doi.org/10.1097/JU.0000000000003481.
Matz, Ethan L, Amy M Pearlman, and Ryan P Terlecki. “Safety and Feasibility of Platelet Rich Fibrin Matrix Injections for Treatment of Common Urologic Conditions.” Investigative and Clinical Urology 59, no. 1 (January 2018): 61–65. https://doi.org/10.4111/icu.2018.59.1.61.
———. “Safety and Feasibility of Platelet Rich Fibrin Matrix Injections for Treatment of Common Urologic Conditions.” Investigative and Clinical Urology 59, no. 1 (January 2018): 61–65. https://doi.org/10.4111/icu.2018.59.1.61.
Matz, Ethan L., Kyle Scarberry, and Ryan Terlecki. “Platelet-Rich Plasma and Cellular Therapies for Sexual Medicine and Beyond.” Sexual Medicine Reviews 10, no. 1 (January 2022): 174–79. https://doi.org/10.1016/j.sxmr.2020.07.001.
Poulios, Evangelos, Ioannis Mykoniatis, Nikolaos Pyrgidis, Filimon Zilotis, Paraskevi Kapoteli, Dimitrios Kotsiris, Dimitrios Kalyvianakis, and Dimitrios Hatzichristou. “Platelet-Rich Plasma (PRP) Improves Erectile Function: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial.” Journal of Sexual Medicine 18, no. 5 (May 1, 2021): 926–35. https://doi.org/10.1016/j.jsxm.2021.03.008.
Raheem, Amr Abdel, Giulio Garaffa, Tarek Abdel Raheem, Michelle Dixon, Amanda Kayes, Nim Christopher, and David Ralph. “The Role of Vacuum Pump Therapy to Mechanically Straighten the Penis in Peyronie’s Disease.” BJU International 106, no. 8 (2010): 1178–80. https://doi.org/10.1111/j.1464-410X.2010.09365.x.
Ruffo, A., M. Franco, E. Illiano, and N. Stanojevic. “Effectiveness and Safety of Platelet Rich Plasma (PrP) Cavernosal Injections plus External Shock Wave Treatment for Penile Erectile Dysfunction: First Results from a Prospective, Randomized, Controlled, Interventional Study.” European Urology Supplements 18, no. 1 (March 2019): e1622–23. https://doi.org/10.1016/S1569-9056(19)31175-3.
Schirmann, A., E. Boutin, A. Faix, and R. Yiou. “Pilot Study of Intra-Cavernous Injections of Platelet-Rich Plasma (P-Shot®) in the Treatment of Vascular Erectile Dysfunction.” Progrès En Urologie, June 2022, S1166708722001300. https://doi.org/10.1016/j.purol.2022.05.002.
Shaher, Hussein, Abdallah Fathi, Salah Elbashir, Shabieb A. Abdelbaki, and Tarek Soliman. “Is Platelet Rich Plasma Safe And Effective In Treatment Of Erectile Dysfunction? Randomized Controlled Study.” Urology, February 2023, S0090429523000742. https://doi.org/10.1016/j.urology.2023.01.028.
Siroky, Mike B., and Kazem M. Azadzoi. “Vasculogenic Erectile Dysfunction: Newer Therapeutic Strategies.” Journal of Urology 170, no. 2S (August 2003). https://doi.org/10.1097/01.ju.0000075361.35942.17.
Towe, Maxwell, Akhil Peta, Russell G. Saltzman, Navin Balaji, Kevin Chu, and Ranjith Ramasamy. “The Use of Combination Regenerative Therapies for Erectile Dysfunction: Rationale and Current Status.” International Journal of Impotence Research, July 12, 2021, 1–4. https://doi.org/10.1038/s41443-021-00456-1.
Researchers (Masterson, 2023) recently used a protocol (that differs from the P-Shot® procedure) and measured the effect on erectile function of injections of the penis with platelet-rich plasma (PRP).
Before reviewing their research and their deviations from the P-Shot® protocol, consider what the P-Shot® is: The P-Shot® (Priapus Shot®) is a service mark that names a procedure that requires training in the standard protocol and an agreement to follow the protocol that has been used (with improvements) for the past 13 years.
The ways Masterson, et al changed the procedure (from that of the P-Shot® procedure) for their study include at least all of the following:
They used a different injection technique than what is used with the P-Shot® procedure; their technique limited the exposure of the penis to less than 1/2 of the tissue treated by the P-Shot® procedure.
They used a centrifuge that is not on the recommended list of devices approved by the FDA for the preparation of PRP for injection back into the body. Their centrifuge also differs from what was used in other studies that showed benefits. The centrifuge used can have dramatic effects on not only the number of platelets but also the number of white blood cells and red blood cells in the sample–all of which is important in regard to results.
They injected 1/2 the volume of PRP usually injected. They injected a total of 5 cc instead of 10 or more cc’s. So not only did their injection technique limit the distribution, but the volume injected limited the treatment area and the number of platelets.
1. They calculated sample size based on the assumption that the placebo group would have a 15% rate of attaining MCID, not the observed 50%; so the study was grossly underpowered and conclusions invalid. Still, we can look at more…
2. Even though they saw less response (with their altered protocol) than what has been shown in other studies, they still saw improvement in erectile function after injection of PRP; the change was just not significantly greater than saline. Both showed improvement.
4. In previous double-blind, placebo studies of PRP for ED, PDE5is were discontinued. In one study, the placebo response (still using saline) was only 15%. Masterson, et al allowed participants to continue their Viagra drugs, which could account for the higher placebo response. The high placebo response also attenuates the power of the study.
5. The study is also compromised mathematically by a 15% dropout rate in an already small sample size.
6. In their introduction, Masterson et. al writes the following: “Even without supporting data, numerous clinics in the largest metropolitan areas of the United States are charging patients for PRP treatments for ED.”
Yet, there IS “supporting data.” Previous studies indeed have shown that PRP does help with ED and with Peyronie’s disease One of those studies was even done by Dr. Ronald Virag, the pioneer in urology who came up with the idea that became “tri-mix” injections for erection and changed urology forever.
The near disappearance of plaque seen in Peyronie’s disease after injection with PRP (Virag, 2017)
The authors failed to recognize all of those studies by stating there is “no supporting data.”
7. They do, later in their discussion, contradict/correct their own statement (“no supporting data”) by making reference to two of many articles that support the P-Shot® procedure and the injection of PRP for ED.
8. Also, the authors fail to point out, in their worries about the money being charged, that the P-Shot® procedure has fewer side effects than Viagra (which has been shown to cause blindness in some) and its cousin drugs and that the cost of a P-Shot® can be less than pharmaceutical alternatives (over time), much less invasive and less expensive than a penile implant, and that P-Shot® providers have agreed to refund the money of anyone not helped by the procedure.
The P-Shot® in no way makes these alternative treatments not useful and needed. But, the P-Shot® should be part of the tools available for treatment, and a man should be able to try the P-Shot® before proceeding to implant.
9. Moreover, the Priapus Shot® procedure is NOT just to give a shot. The procedure includes an evaluation to see if the shot is appropriate. There must be phlebotomy (usually another skilled employee’s time and expense) and processing of blood using FDA kits approved for processing blood for autologous reinjection (not cheap). The cost to the patient helps covers these expenses.
10. Other studies have shown a greater improvement in erectile function than what was seen by these authors. So, we are grateful for their contribution–showing that a different protocol works less well. Further studies are needed to look at the variables regarding the preparation of the PRP, activation, and injection technique to understand further why their protocol was less effective and how current protocols can be improved.
Some of the supporting data for PRP for the treatment of ED.
In conclusion, Masterson et al demonstrated (in this underpowered study using a placebo that is not a placebo) that injecting 1/2 the volume of the P-Shot® procedure using their alternative technique of injecting and not activating the PRP with CaCl is possibly less effective than what has been shown in other studies. That is valuable to know, and we are grateful for their study.
References Regarding the Benefits of the P-Shot® Procedure for ED
Bosma-Den Boer, Margarethe M., Marie Louise Van Wetten, and Leo Pruimboom. “Chronic Inflammatory Diseases Are Stimulated by Current Lifestyle: How Diet, Stress Levels and Medication Prevent Our Body from Recovering.” Nutrition and Metabolism 9 (2012). https://doi.org/10.1186/1743-7075-9-32.
Casabona, Francesco, Ilaria Gambelli, Federica Casabona, Pierluigi Santi, Gregorio Santori, and Ilaria Baldelli. “Autologous Platelet-Rich Plasma (PRP) in Chronic Penile Lichen Sclerosus: The Impact on Tissue Repair and Patient Quality of Life.” International Urology and Nephrology 49, no. 4 (April 2017): 573–80. https://doi.org/10.1007/s11255-017-1523-0.
Chung. “A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction.” Medical Sciences 7, no. 9 (August 29, 2019): 91. https://doi.org/10.3390/medsci7090091.
Chung, Eric. “Medical Sciences A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction,” 2019, 1–11.
Everts, Peter, Kentaro Onishi, Prathap Jayaram, José Fábio Lana, and Kenneth Mautner. “Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020.” International Journal of Molecular Sciences 21, no. 20 (October 21, 2020): 7794. https://doi.org/10.3390/ijms21207794.
Garcia, MM, TM Fandel, G Lin, AW Shindel, L Banie, CS Lin, and TF Lue. “Treatment of Erectile Dysfunction in the Obese Type 2 Diabetic ZDF Rat with Adipose Tissue-Derived Stem Cells,” 2010, 14.
Israeli, Joseph M., Soum D. Lokeshwar, Iakov V. Efimenko, Thomas A. Masterson, and Ranjith Ramasamy. “The Potential of Platelet-Rich Plasma Injections and Stem Cell Therapy for Penile Rejuvenation.” International Journal of Impotence Research, November 6, 2021, 1–8. https://doi.org/10.1038/s41443-021-00482-z.
Kumar, C.S. “265 Combined Treatment of Injecting Platelet Rich Plasma With Vacuum Pump for Penile Enlargement.” The Journal of Sexual Medicine 14, no. 1 (January 2017): S78. https://doi.org/10.1016/j.jsxm.2016.11.174.
Liu, Ming-Che, Meng-Lin Chang, Ya-Chun Wang, Wei-Hung Chen, Chien-Chih Wu, and Shauh-Der Yeh. “Revisiting the Regenerative Therapeutic Advances Towards Erectile Dysfunction.” Cells 9, no. 5 (May 19, 2020): 1250. https://doi.org/10.3390/cells9051250.
Matz, Ethan L, Amy M Pearlman, and Ryan P Terlecki. “Safety and Feasibility of Platelet Rich Fibrin Matrix Injections for Treatment of Common Urologic Conditions.” Investigative and Clinical Urology 59, no. 1 (January 2018): 61–65. https://doi.org/10.4111/icu.2018.59.1.61.
Matz, Ethan L., Kyle Scarberry, and Ryan Terlecki. “Platelet-Rich Plasma and Cellular Therapies for Sexual Medicine and Beyond.” Sexual Medicine Reviews 10, no. 1 (January 2022): 174–79. https://doi.org/10.1016/j.sxmr.2020.07.001.
Poulios, Evangelos, Ioannis Mykoniatis, Nikolaos Pyrgidis, Filimon Zilotis, Paraskevi Kapoteli, Dimitrios Kotsiris, Dimitrios Kalyvianakis, and Dimitrios Hatzichristou. “Platelet-Rich Plasma (PRP) Improves Erectile Function: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial.” Journal of Sexual Medicine 18, no. 5 (May 1, 2021): 926–35. https://doi.org/10.1016/j.jsxm.2021.03.008.
Raheem, Amr Abdel, Giulio Garaffa, Tarek Abdel Raheem, Michelle Dixon, Amanda Kayes, Nim Christopher, and David Ralph. “The Role of Vacuum Pump Therapy to Mechanically Straighten the Penis in Peyronie’s Disease.” BJU International 106, no. 8 (2010): 1178–80. https://doi.org/10.1111/j.1464-410X.2010.09365.x.
Ruffo, A., M. Franco, E. Illiano, and N. Stanojevic. “Effectiveness and Safety of Platelet Rich Plasma (PrP) Cavernosal Injections plus External Shock Wave Treatment for Penile Erectile Dysfunction: First Results from a Prospective, Randomized, Controlled, Interventional Study.” European Urology Supplements 18, no. 1 (March 2019): e1622–23. https://doi.org/10.1016/S1569-9056(19)31175-3.
Schirmann, A., E. Boutin, A. Faix, and R. Yiou. “Pilot Study of Intra-Cavernous Injections of Platelet-Rich Plasma (P-Shot®) in the Treatment of Vascular Erectile Dysfunction.” Progrès En Urologie, June 2022, S1166708722001300. https://doi.org/10.1016/j.purol.2022.05.002.
Shaher, Hussein, Abdallah Fathi, Salah Elbashir, Shabieb A. Abdelbaki, and Tarek Soliman. “Is Platelet Rich Plasma Safe And Effective In Treatment Of Erectile Dysfunction? Randomized Controlled Study.” Urology, February 2023, S0090429523000742. https://doi.org/10.1016/j.urology.2023.01.028.
Siroky, Mike B., and Kazem M. Azadzoi. “Vasculogenic Erectile Dysfunction: Newer Therapeutic Strategies.” Journal of Urology 170, no. 2S (August 2003). https://doi.org/10.1097/01.ju.0000075361.35942.17.
Towe, Maxwell, Akhil Peta, Russell G. Saltzman, Navin Balaji, Kevin Chu, and Ranjith Ramasamy. “The Use of Combination Regenerative Therapies for Erectile Dysfunction: Rationale and Current Status.” International Journal of Impotence Research, July 12, 2021, 1–4. https://doi.org/10.1038/s41443-021-00456-1.
Masterson, Thomas A., Manuel Molina, Braian Ledesma, Isaac Zucker, Russell Saltzman, Emad Ibrahim, Sunwoo Han, Isildinha M. Reis, and Ranjith Ramasamy. “Platelet-Rich Plasma for the Treatment of Erectile Dysfunction: A Prospective, Randomized, Double-Blind, Placebo-Controlled Clinical Trial.” Journal of Urology, April 30, 2023, 10.1097/JU.0000000000003481. https://doi.org/10.1097/JU.0000000000003481.
References Regarding P-Shot® Procedure for Peyronie’s Disease
Culha, Mehmet Gokhan, Erkan Erkan, Tugce Cay, and Uğur Yücetaş. “The Effect of Platelet-Rich Plasma on Peyronie’s Disease in Rat Model.” Urologia Internationalis 102, no. 2 (2019): 218–23. https://doi.org/10.1159/000492755.
Raheem, Amr Abdel, Giulio Garaffa, Tarek Abdel Raheem, Michelle Dixon, Amanda Kayes, Nim Christopher, and David Ralph. “The Role of Vacuum Pump Therapy to Mechanically Straighten the Penis in Peyronie’s Disease.” BJU International 106, no. 8 (2010): 1178–80. https://doi.org/10.1111/j.1464-410X.2010.09365.x.
Virag, Ronald, Hélène Sussman, Sandrine Lambion, and Valérie de Fourmestraux. “Evaluation of the Benefit of Using a Combination of Autologous Platelet Rich-Plasma and Hyaluronic Acid for the Treatment of Peyronie’s Disease.” Sexual Health Issues 1, no. 1 (2017). https://doi.org/10.15761/SHI.1000102.
References Regarding Saline is Not a Placebo
Asghar, Aneela, Zahid Tahir, Aisha Ghias, Usma Iftikhar, and Tahir Jameel Ahmad. “Efficacy and Safety of Intralesional Normal Saline in Atrophic Acne Scars.” Annals of King Edward Medical University 25, no. 2 (June 24, 2019). https://doi.org/10.21649/akemu.v25i2.2867.
Bagherani, Nooshin, and Bruce R Smoller. “Introduction of a Novel Therapeutic Option for Atrophic Acne Scars: Saline Injection Therapy.” Global Dermatology 2, no. 6 (2016). https://doi.org/10.15761/GOD.1000159.
Bokey, E. L., J. P. Keating, and P. Zelas. “HYDRODISSECTION: AN EASY WAY TO DISSECT ANATOMICAL PLANES AND COMPLEX ADHESIONS.” ANZ Journal of Surgery 67, no. 9 (September 1997): 643–44. https://doi.org/10.1111/j.1445-2197.1997.tb04616.x.
Cass, Shane P. “Ultrasound-Guided Nerve Hydrodissection: What Is It? A Review of the Literature” 15, no. 1 (2016): 3.
“Clinical Benefit of Intra-Articular Saline as a Comparator in Clinical Trials of Knee Osteoarthritis Treatments_ A Systematic Review and Meta-Analysis of Randomized Trials | Elsevier Enhanced Reader.” Accessed April 6, 2022. https://doi.org/10.1016/j.semarthrit.2016.04.003.
El-Amawy, Heba Saed, and Sameh Magdy Sarsik. “Saline in Dermatology: A Literature Review.” Journal of Cosmetic Dermatology 20, no. 7 (2021): 2040–51. https://doi.org/10.1111/jocd.13813.
Popp, Lothar W. “Improvement in Endoscopic Hernioplasty: Transcutaneous Aquadissection of the Musculofascial Defect and Preperitoneal Endoscopic Patch Repair.” Journal of Laparoendoscopic Surgery 1, no. 2 (January 1991): 83–90. https://doi.org/10.1089/lps.1991.1.83.
Saltzman, Bryan M., Timothy Leroux, Maximilian A. Meyer, Bryce A. Basques, Jaskarndip Chahal, Bernard R. Bach, Adam B. Yanke, and Brian J. Cole. “The Therapeutic Effect of Intra-Articular Normal Saline Injections for Knee Osteoarthritis: A Meta-Analysis of Evidence Level 1 Studies.” The American Journal of Sports Medicine 45, no. 11 (September 1, 2017): 2647–53. https://doi.org/10.1177/0363546516680607.
Searle, Tamara, Firas Al-Niaimi, and Faisal R. Ali. “Saline in Dermatologic Surgery.” Journal of Cosmetic Dermatology 20, no. 4 (2021): 1346–47. https://doi.org/10.1111/jocd.13996.
Sharma, ReenaK, Mudita Gupta, and Ritu Rani. “Delineating Injectable Triamcinolone-Induced Cutaneous Atrophy and Therapeutic Options in 24 Patients—A Retrospective Study.” Indian Dermatology Online Journal 13, no. 2 (2022): 199. https://doi.org/10.4103/idoj.idoj_483_21.
References Regarding the Activation of PRP
Hamilton, Bruce, Johannes L. Tol, Wade Knez, and Hakim Chalabi. “Exercise and the Platelet Activator Calcium Chloride Both Influence the Growth Factor Content of Platelet-Rich Plasma (PRP): Overlooked Biochemical Factors That Could Influence PRP Treatment.” British Journal of Sports Medicine 49, no. 14 (July 1, 2015): 957–60. https://doi.org/10.1136/bjsports-2012-091916.
Kao, David S., Stephanie W. Zhang, and Alexander R. Vap. “A Systematic Review on the Effect of Common Medications on Platelet Count and Function: Which Medications Should Be Stopped Before Getting a Platelet-Rich Plasma Injection?” Orthopaedic Journal of Sports Medicine 10, no. 4 (April 1, 2022): 232596712210888. https://doi.org/10.1177/23259671221088820.
Sheean, Andrew J., Adam W. Anz, and James P. Bradley. “Platelet-Rich Plasma: Fundamentals and Clinical Applications.” Arthroscopy: The Journal of Arthroscopic & Related Surgery 37, no. 9 (September 2021): 2732–34. https://doi.org/10.1016/j.arthro.2021.07.003.
Smith, Oliver J., Selim Talaat, Taj Tomouk, Gavin Jell, and Ash Mosahebi. “An Evaluation of the Effect of Activation Methods on the Release of Growth Factors from Platelet-Rich Plasma.” Plastic and Reconstructive Surgery 149, no. 2 (February 2022): 404–11. https://doi.org/10.1097/PRS.0000000000008772.
Smith, Stephanie A., Richard J. Travers, and James H. Morrissey. “How It All Starts: Initiation of the Clotting Cascade.” Critical Reviews in Biochemistry and Molecular Biology 50, no. 4 (July 4, 2015): 326–36. https://doi.org/10.3109/10409238.2015.1050550.
Toyoda, Toshihisa, Kazushige Isobe, Tetsuhiro Tsujino, Yasuo Koyata, Fumitaka Ohyagi, Taisuke Watanabe, Masayuki Nakamura, et al. “Direct Activation of Platelets by Addition of CaCl2 Leads Coagulation of Platelet-Rich Plasma.” International Journal of Implant Dentistry 4 (August 1, 2018): 23. https://doi.org/10.1186/s40729-018-0134-6.
Ulasli, Alper Murat, Gokhan Tuna Ozturk, Bagdagul Cakir, Gulsemin Erturk Celik, and Fatih Bakir. “The Effect of the Anticoagulant on the Cellular Composition and Growth Factor Content of Platelet-Rich Plasma.” Cell and Tissue Banking, August 28, 2021. https://doi.org/10.1007/s10561-021-09952-6.
The information provided by Shahinyan et al. does, however, warrant clarification—which is the purpose of this memorandum. I will review their article in the order in which it was written and cover all of the following:
PRP & ED history
The need for standardization
Service marks and trademarks
Shahinyan missed the mark
More PRP history (and how it led to the P-Shot® procedure)
Seeking the “Novel Cure” or the “New Penis”?
Testicles are a “fad”
Methods of spying “secret shopping”
A “New Transmission” or a “New Penis”?
Guidelines: a 4-year update
Physicians & Non-Physicians
Guidelines & “Consumerization-Driven” Cattle
Advertising: Noble or Evil?
Have you seen a picture of “These”?
What do PRP, Shock Wave, and Stem Cells Share?
Limitations & Corrections
Future research
References
Though I was the first to perform the P-Shot® procedure (when I designed it in 2010), that would be worth nothing without the brilliant work of the members of our group, the Cellular Medicine Association (CMA); we need more thought leaders and brave clinicians determined to improve health, sexual relations, and families worldwide. I hope you will join us. Sincerely, Charles Runels, MD Inventor of the P-Shot® procedureCellular Medicine AssociationDrRunels@Runels.com 1-888-920-5311
To clarify the discussion of the article in JAMA about the P-Shot® procedure, first consider the science and history of PRP injections into the penis for the treatment of ED.
PRP & ED History
As early as 2003, Mike Siroky pointed out in the Journal of Urology that “current therapy, while effective in circumventing vasculogenic ED, is relatively ineffective in permanently reversing the condition. Further research aimed at long-term treatment strategies in vasculogenic ED is needed [Siroky2003].”
For example, phosphodiesterase type 5 inhibitors (PDE5Is), alprostadil injections, and penile implants, all “circumvent” the neurovascular disease that causes most ED; they only help the diseased tissue to better function to achieve a harder erection without improving the health of the tissue. As ED progresses over time, all existing pharmaceutical therapies become less effective–requiring escalating doses, and risking more side effects, leaving the underlying disease process unchecked–until eventually, the drugs cease to work at all.
To avoid this unwanted progression, Siroky also described (in the same 2003 article) a number of therapies that show promise to actually slow or reverse the disease process of ED; one of those therapies he described as follows: “Neovascularization using vascular growth factors has recently been demonstrated to be feasible in animal models.” [Siroky and Azadzoi, 2003, p. 24].
The growth factors to which Dr. Siroky referred in 2003 (that cause neovascularization and neurogenesis) are found in PRP. Nineteen years later, should we not be implementing this knowledge in the clinic if possible?
These same growth factors, to which Dr. Garcia referred in 2010 (that can increase nitric oxide in the dorsal nerve and improve corpus cavernosi architecture), can be found in PRP. Twelve years later, should we not be implementing this knowledge in the clinic if possible?
This same year, in 2010, twelve years ago, after reading these as well as other studies of PRP in the arena of wound care and in the facial-aesthetics arena (specifically those by Dr. Sclafani and others showing neovascularization and neurogenesis), Charles Runels, as a way of thinking about the treatment of ED with PRP, first explored the use of PRP in facial aesthetics—using a very specific method of injecting hyaluronic acid (HA) fillers combined with injecting PRP as part of the same procedure–which he registered in 2010, Vampire Facelift®, US Patent & Trademark Office (Reg #85127646). Then, after actually seeing successful neovascularization in the face that occurred after injection with PRP (increased rubor and turgor), Runels extended these ideas and developed a specific method for injecting PRP into the penis for the treatment of ED.
So, in 2010, the author of this memorandum (Charles Runels, MD), was first to inject the human penis with PRP (both the PRP & the penis were his own). Then, seeing improvement in both penile size and function, he further developed the technique in the treatment of his own patients; later in 2010, he registered his idea with the US Patent & Trademark Office (USPTO) for definition and protection of the specific method: using the name Priapus Shot® (Reg#3965320), he defined for the USPTO the procedure as a specific “medical procedure using blood-derived growth factors including platelet-rich fibrin matrix to enhance the size or function of the penis.” He then registered a synonym for the Priapus Shot®, the P-Shot® (Reg#4820964).
Other considerations that prompted that first injection in 2010 by Runels included his practice at a hospital-based wound care center, practicing facial aesthetics with HA fillers, and caring for over three thousand menopausal women and andropausal men who had come to his private internal medicine practice for help with sexual relations.
Because of this mix of offerings in his practice, and seeing the non-standard, unpredictable ways in which facial aesthetics are done, Runels also recognized, in 2010, the need for the standardization of how PRP might be injected into the penis.
The Need for Standardization
To understand the need for standardization of PRP-injection techniques for the treatment of ED, by analogy, consider the situation in 2010 (when Runels developed the P-Shot®) and ongoing with the injection of HA fillers (like Juvederm® or Restylane®) for aesthetic purposes: as of yet, there is still, in 2022, no standardization of methods for the injection of HA fillers—none. Also, there is stillno medical board that governs how HA fillers are injected.
The techniques for the injection of HA fillers vary so much that women often fear that, should they undergo treatment, they will be made to look “weird” or grow “duck lips.” Moreover, with the improper injection of HAs, one risks a significant danger of blindness, skin necrosis, and pulmonary emboli.
Even with these serious risks associated with the injection of HA fillers, the license required to inject HAs varies greatly from state to state; for example, in Alabama, only MDs or DOs can inject HA fillers; in some states, an RN can inject them with physician supervision; in some states, nurse practitioners can inject them with supervision but RN’s cannot; in some states, nurse practitioners can both inject HA fillers and practice medicine (writing prescriptions for complicated medical patients on multiple medications with multiple organs failing)—without any physician supervision at all.
Seeing the large variety of injection techniques and the inconsistent licensing required in the facial aesthetics arena prompted Runels to anticipate that the same variability could happen with the injection of PRP for sexual dysfunction and that such variability could create a dangerous problem; so, that is the reason when he registered his ideas with the USPTO that he filed for a particular type of protective trademark, a “service mark”: Priapus Shot® (P-Shot®) is a type of trademark, a service mark, which provides and demands standardization regarding a specific method of doing.
Service Marks & Trademarks
A “service mark” defines a specific method of doing something and then provides an ongoing legal mechanism to assure that anyone using that service mark in advertising is using that same method; this is different from a “trademark” which defines a specific material or device: for example, Juvederm®, is a trademark which identifies a material, with no indication of the method of injecting that material; Vampire Faceilft®, however, is a “service mark,” which identifies a specific method of injecting (that includes how PRP and HA are prepared and injected), but does not indicate simply a specific material.
The very existence and continued protection of the service mark, P-Shot® (and its synonym, Priapus Shot®), is the reason it is inaccurate to cluster, in the JAMA article under consideration, both those who advertise only PRP (a material) injections for the penis (with no standardization of either preparation or injection) together with those who advertise the P-Shot® procedure (which demands a specific method, including the standardizationall of the following: PRP preparation, injection techniques, patient selection, as well as standardized protocols for pre and post-procedure, and specific financial policies in regards to protecting the patient.
For the standardization of the medical license required to qualify for training to do the P-Shot® and the further training required to offer the P-Shot® procedure, the policy of the Cellular Medicine Association (which oversees the licensing of the P-Shot® trademark and currently enjoys the collaborative efforts of over 3,600 physicians and their extenders in over 55 countries) established the policy that the license to inject PRP under the trademarked names (P-Shot® or Priapus Shot®) will mirror for each state the policy within each state regarding the license to inject HA fillers. This policy would apply to anyone legally using the name P-Shot® but could not apply to anyone advertising the generic term, “PRP,” since the Cellular Medicine Association (CMA) has no legal ability to patrol a generic term (PRP).
To continue the analogy, in regards to HA fillers, the marketing to consumers of Juvederm® and other HA fillers does nothing more than identifying the material to be injected (not the method of injection).
Advertisements by both manufacturers (such as Allergan) and physicians who offer HA fillers essentially say, “Come here for your Juvederm,” with no indication of the method to be used for injecting the Juvederm.
Even if one chooses a provider of HA fillers based on board certification (for example, going to someone boarded in plastic surgery), the injector in the plastic surgeon’s office may be an RN physician extender (no prediction of the license of the injector) and the injection technique will likely also vary from office to office.
Shahinyan missed the Mark
Since Shahinyan et al. did not make the distinction between surveying those advertising PRP (a material) and those advertising the P-Shot® procedure–a specific and legally-defined method (service mark) involving patient selection, monetary policy, preparation of PRP, and a method of injection of PRP), and instead equated all of the clinics (whether advertising a material or a method), and since the authors failed to use the ® mark to acknowledge the servicemark, P-Shot®(demonstrating that the authors were blind to the mark and to its purpose), most of the conclusions in their paper become suspect at best.
Ironically, the P-Shot® procedure methodology solves the very problems (method standardization and provider qualification) that Shahinyan et al lament is lacking in the clinics they secret shopped. To further understand their article and the P-Shot® procedure, consider more about the history of PRP.
More PRP History
Autologous-derived PRP has been used for decades by dentists, orthopedic surgeons, and others dealing with difficult-to-treat wounds in order to promote post-op tissue healing. Platelets are naturally activated as part of the thrombin cascade to release their growth factors whenever an injury occurs (including with every surgery); with this activation is formed platelet-rich fibrin matrix (PRFM) which holds in place the growth factors and chemotactic factors released from platelets—recruiting and activating local and distant pluripotent stem cells to grow new and healthier tissue.
The reason the orthopedists and dentists were interested in PRP before urologists, gynecologists, and most facial plastic surgeons took note of PRP is because orthopedists and dentists routinely deal with completely or near completely avascular tissue and so they were looking for ways to improve post-op recovery in hard-to-heal tissue by injecting into avascular tissue the growth factors that would be in the blood and promote healing if the tissue were vascular. So, the devices that are now FDA-cleared to prepare PRP for injection back into the body and that are being used for the preparation of PRP for injection into the face and into the genitalia of both men and women, these devices were researched and developed in the arenas of dentistry and orthopedics for two decades before being brought into the sexual medicine arena.
The Left Specialty Not Knowing What the Right Specialty is Doing
As another example of the uneven progress of medicine between different specialties, consider the following: gynecologists were using endoscopic surgery for years while the general surgeons largely ignored the tool; hysterectomy was done endoscopically for years before cholecystectomy. The general surgeons only became proficient with endoscopic surgery after Dr. Bill Seay (a gynecologist) demonstrated that an endoscopic cholecystectomy is feasible and safe, and then widely taught the technique to general surgeons. Before Dr. Seay’s innovation, the proverbial left-hand-specialty was unaware of what the right-hand-specialty was doing. In the same way, dentists and orthopedic surgeons, and bench scientists successfully used and determined much of the methodology of PRP before most urologists became even aware of the tool’s existence.
In summary, the use of autologously-harvested platelets enriched in numbers within the patient’s own plasma (PRP) and then injected into damaged or diseased tissue to encourage the growth of healthier tissue is not “homeopathy” or “alternative” medicine (as suggested by the JAMA article under review), it is just “medicine”—employing well-known principles of wound care to improve tissue health and function. What has become standard medicine within one specialty can seem questionable when first brought to another specialty.
other uses of PRP that have evolved from the work of dentists & orthopedic surgeons:
The care of a sternal wound (post-CABG);
To promote healing of and to fight the infection of ulcers of the distal extremities;
To treat alopecia areata;
To control pain;
To improve function and slow degeneration in osteoarthritis of the knee;
To remodel acne scars;
To soften nasolabial folds and create a younger-appearing face;
To promote hair growth;
To help recovery from Bell’s Palsy;
To treat urinary incontinence in women;
To treat interstitial cystitis;
To help with the harvest of viable eggs in a postpartum woman;
To help with pain and healing post mesh placement in women.
The list is potentially as extensive as the need for healthier tissue.
All of the above-referenced uses are supported by research; and, all of these uses are both autologous and homologous (in keeping with the body’s natural function in regards to platelet-derived growth factors) and so are not governed by the FDA (the FDA does not govern hair, blood, urine, and skin—those are ‘minimally manipulated” and belong to the patient; the procedures done with these tissues and with PRP are the business of doctors, not the FDA).
The authors of the JAMA article state that “guidelines from professional societies, such as the American Urological Association…classify PRP as investigational and not to be provided for payment.” [Shahinyan et al., 2022, p. 1] Yet, the guidelines referenced were written 4 years ago. And, body tissues (like hair & skin grafts, & PRP) are not investigational, they just are. Moreover, the use of platelet-derived growth factors for the propagation of healthier tissue in the penis, with a resultant improvement in erectile function, is supported by research that has grown significantly since the publication of the 4-years-old guidelines referenced by Shhinyan et al.
Before looking more closely at the more current research, the idea of what is “novel” should be considered, since that word is how PRP is described in the JAMA article under review.
Seeking the “Novel Cure” or the “New Penis”?
The authors report in JAMA that the P-Shot® procedure is marketed to men looking for “novel cures.” Since the authors “secret shopped” the clinics, not the patients of the clinics, it seems they used clairvoyance rather than research to determine the volition of menwho receive PRP for ED at these clinics.
Since P-Shot® providers do, in fact, survey their patients, we can state (without assuming) that men who receive the P-Shot® procedure are educated enough to not be duped into being “driven” to treatment simply because it is “novel”; when men seek a P-Shot® procedure, what they want is not a “novel” treatment but a “new penis”: a harder erection by improving the health of the penis (instead of a ‘bandaid’ that improves function for the night but that neither addresses nor slows the progression of the underlying neurovascular pathology).
This goal of a new penis is in keeping with the goals stated by Dr. Siroky in the 2003 Journal of Urology article previously referenced.
Instead of “novel,” men want something that “works” without the risk of blindness or stroke or the inconvenience of headache or the pain of a penis shot of vasodilators as part of foreplay, or surgery, or the lifetime expense of medicines (over time, such expense is greater with the PDE5Is than with an occasional P-Shot®).
Testicles are a “Fad”
The authors also mention, as an analogy to PRP, the recent growth of the numbers of men seeking testosterone replacement, calling the trend of increasing numbers of men seeking testosterone a “health fad” that resulted from “direct-to-consumer marketing.”
Stating that testosterone replacement for men grew in popularity solely as a health fad without mentioning the simultaneous explosion of research supporting the ways testosterone replacement may benefit an andropausal man could be discussed at length; but, since that would require a textbook, I will forgo that discussion and simply notice that the direct-to-consumer marketing of PRP mentioned by the authors is dwarfed beyond comparison by the mammoth amount of money spent in direct-to-consumer marketing of phosphodiesterase 5 inhibitors (PDE5Is).
It is unlikely that one will ever see an ad for PRP on sports TV because there can be no patent on a person’s blood, therefore there can be no profit made regarding PRP by pharmaceutical companies—the only for-profit entity in medicine that can afford such expensive advertising.
The mammoth amount of money spent in direct-to-consumer marketing PDE5Is is not undesired. Drugs are not bad, drugs save lives. Even profit is not evil; pharmaceutical companies need profit to afford the research that finances the discovery of new drugs, and new drugs save lives. Physicians also need profit to pay for their staff, their children, their car to get to work, new books, the lights at their office, and their malpractice insurance. But, in regards to the JAMA article under discussion, the amount of profit being made and the amount of advertising being financed in regards to PDE5Is is mammoth beyond comparison with the profit and advertising associated with PRP, so much so that one may wonder why the miniscule marketing budget of private physicians is even a topic of discussion.
Furthermore, even though the advertising dollars spent by companies advertising PDE5Is dwarfs the advertising dollars spent by physicians educating their patients about the P-Shot®, the whole issue seems irrelevant, since one will find no significant research showing that the amount of money spent on advertising correlates (either negatively or positively) with either the effectiveness of or the need for any particular treatment.
In further discussions of profit, the authors mention their previous paper regarding the prescribing of testosterone without patient examination; the point is without question—testosterone should not be prescribed without a true history and physical exam. But, this point is again irrelevant to the P-Shot® procedure since by definition there must be an in-person encounter for the patient to undergo the procedure.
If the motivation of Shahinyan et al in mentioning profits and price in regards to the P-Shot® procedure does not relate to the quality of care (and it seems that it does not), then their discussion of profit takes the tone of labeling profits made by physicians to be unethical (while ignoring the profits made by pharmaceutical companies). Most likely, the intention of the authors was neither malicious nor uninformed; perhaps (though here I am also succumbing to clairvoyance), such views of profit from procedures not covered by insurance could be the inevitable, unconscious worldview of authors who (as stated with their conflict-of-interest disclosures) are fed by the payroll of pharmaceutical companies. Most physicians (including most P-Shot® providers) are not thus fed.
Spying “Secret Shopper” Methods
Before going further, the methods of the JAMA authors should be considered: they used “secret shopper methods” (Shahinyan et al., 2022, p. 1.
As mentioned previously, even though they included providers of the P-Shot® procedure in their analysis, their “secret shopper methods” included PRP injectors not found in the P-Shot® provider directory.
Restated, they secret shopped providers of PRP who do not use the P-Shot® name or methodologies as well as those who do follow P-Shot® methodologies.
But, those who do not use the P-Shot® name do not follow a standardized method, and those who do use the P-Shot® name do follow a standardized method. Moreover, even when they “secret shopped” those using the P-shot® name in advertising, there is no mention of whether they checked to see if the person using the name is actually licensed (by the Cellular Medicine Association) to use the name in advertising—this is a critical point to consider when understanding the limitations and conclusions of the study.
In summary, the study defined an apples and oranges group; but the study’s assumptions and conclusions apply only to the apples. Two of the endpoints of the authors, the standardization and licensing of the providers, are not controlled in any way in the advertising of PRP; but, both of those variables are controlled in those offering the P-Shot® procedure—partly by spending millions on legal fees (by the CMA) to control who advertises with the name P-Shot® and Priapus Shot®. That money is spent both in the herculean efforts of training new providers and the legal battles of forcing the cease and desist outcome in thousands of infringers.
Furthermore, in regards to money and its relation to the patient, those in the CMA who provide the P-Shot® procedure agree to offer a complete money back to anyone who is not helped. Those who simply offer PRP injections often do not provide a refund if the patient is not pleasedby the results of the procedure. So, the worst that could happen with a P-Shot® provider would be most likely only lost time and inconvenience but not lost money (except by the provider who loses the cost of goods and the time it took to care for the patient). But, patients who undergo PRP could be both out of pocket and perhaps even at the risk of serious disease by a provider who does not have the proper license.
In regards to the cost of the procedure to the patient, the amount of money charged is similar to a new set of tires, definitely worth it if it helps (and the money is refunded if it does not help).
And, since the procedure is not yet covered by insurance unless the provider wishes to pay to go to work instead of providing for her family, it is necessary for her to recover her time and cost of goods by charging the patient instead of insurance.
To understand the cost to the provider, consider that the time involved to offer the procedure is not simply to give a shot. Also required is the time and expense of taking a history, often talking with the spouse as well, in addition to time reviewing past medical records, doing phlebotomy, processing the blood to isolate the PRP using an FDA-cleared device (also an expense), and finally doing the injection, followed by phone calls and/or visits to evaluate results and make further recommendations.
A 1-hour massage at a nice hotel is $300 and is provided by someone who attended a six-month class. In contrast, a procedure that might improve relationships and that involves an expensive FDA-cleared device, and the time and skills needed to evaluate the patient, do an exam, draw blood, inject the PRP into the corpus cavernosum, and follow up with the patient are worth more than a massage and probably as much as a new set of tires.
Guidelines: A 4-Year Update
Since Shahinyan et al. also lament the use of PRP “despite a paucity of evidence for its use” but use the word “paucity” without giving reference to the current body of research (so that we may judge whether or not it is indeed pauce), it may be helpful to fill that omission with an overview of the evidence regarding PRP and ED that has developed since the author’s referenced opinion (issued 4 years ago, in 2018).
Before looking specifically at research regarding ED, consider that PRP research, in general, supplies over 15,000 papers referenced in PubMed–most of which can be ubiquitously extrapolated to other parts of the body.
For example, if you show with biopsy that injecting PRP into the back of the arm results in neovascularization and neurogenesis [Sclafani2012] do you need to do the same study for the front of the arm, for the face, or for the penis? In fact, the reason Sclafani did the study using tissue on the back of the arm is that he was looking for a way to improve the face; since a biopsy of the face would be undesirable, he knew that demonstrating the effects in the arm was enough to allow us to at least extrapolate the possibility of the idea to the face–and the penis.
Such studies that can be extrapolated to the penis to at least indicates possibilities include studies regarding using PRP to treat all of the following: improving scar tissue (which would relate to Peyronie’s disease), wound healing, neovascularization, neurogenesis, downregulation of the auto-immune system (Peyronie’s), muscle repair, and collagen synthesis.
Other important studies that affect the study of PRP include those that show that saline has an effect on tissue growth and repair when used to hydrodissect tissue. The possible therapeutic effect of saline is important since, in research regarding the promotion of healthier tissue, injecting saline is not a good placebo: since saline has an effect on tissue when used for hyrodissection, the measured results of the studied injection technique (i.e. PRP) would be erroneously attenuated if saline is used as a placebo.Blinded placebo studies with PRP, therefore, are considered impossible to do by some investigators because there is a physical component to the hydrodissection (as would be impossible in a blinded study of any surgical procedure). Comparison studies, or perhaps unblinded studies where the placebo is simply inserting the needle without injection, may be the highest level of a comparison study of PRP that can be accurately done.
A sampling of research can be found referenced in the bibliography of this memo. You’ll see papers supporting PRP to help with BXO, Peyronie’s disease, ED, penile rehabilitation post prostate surgery, and urinary incontinence post prostate surgery.
You will also find referenced at the end of this memo a collection of papers demonstrating benefits to women with sexual dysfunction. This was included because the tissue of women and men is identical in many ways: both have corpus cavernosi, corpus spongiosum, a prostate (Skene’s glands), and similar problems with the same nerves and blood flow. Because there are fewer pharmaceutical solutions for women than for men (for example, women still do not have an FDA-approved form of testosterone), there seems to be more PRP research directed toward women; and much of it may eventually be extrapolated to men.
At what point the body of research ceases to be pauce and becomes sufficient to adopt the P-Shot® procedure into an everyday clinic setting will vary from clinician to clinician, like all new ideas, based on the risks of the procedure (almost none with PRP), the logic and science behind the idea (much with PRP), the possible benefits of the procedure (better penis health and stronger family relations), and the amount of supporting research, and the understanding of the clinician of the current research—but there is no clear finish line with any procedure. The usual time frame for the widespread adoption of a new idea is around 20 years (for example the first heart catheterization was done in the 1940s and it took about 20 years for the idea of antibiotics for peptic ulcer disease to become widely adopted).
Some of the determination of when to adopt a new treatment strategy may even vary based on whether it is the doctor who is suffering the social and psychological effects of ED with a disturbing attenuation of the effects of the usual pharmacological solutions, or it is the patient of the doctor who is suffering.
Physicians & Non-Physicians
The authors of the JAMA article under discussion found especially disturbing the “number of nonphysicians” providing PRP for ED. To emphasize what was mentioned earlier in this memo, analogous to hyaluronic acid filler use where in some states like Alabama no physician extenders can do hyaluronic acid filler where in some states RNs can inject hyaluronic acid fillers, there are no definite guidelines about who can inject PRP; so, we thought (at the CMA) the most logical strategy would be to reflect each state’s policy about which license would each state allow to inject hyaluronic acid fillers and then mirror that same official policy with PRP. The logic is that since hyaluronic acid filler injections can cause blindness, necrosis of skin, and pulmonary emboli when injected improperly, and since PRP is not associated with any of these complications, and so is safer than HAs, if we mirrored the HA policies in each state, there should be no objection.
But, there is no such governance of the injection or advertising of PRP as a generic term as we have both adopted and spent millions of dollars enforcing at the CMA.
Particularly confusing, the authors of the JAMA article were also bothered by the number of “physicians with no formal training in male sexual dysfunction, such as gynecologists.” Said another way, “gynecologists have no formal training in caring for men with sexual dysfunction and should not be allowed to do so.”
A number of years ago, ACOG, briefly, ruled that gynecologists should not take care of men–then they reversed that decision. Gynecologists have strong training in general primary care and women often bring their husbands with them to the gynecologist and want their gynecologist to care for them both as a couple. The American Board of Obstetrics and Gynecology, realizing that gynecologists have a deep understanding of endocrinology and in fact do the first male surgery that most men undergo (circumcision), wisely reversed their decision to prevent gynecologists from caring for men and determined that gynecologists are capable of caring for both women and men. The authors of this JAMA article may disagree with the policy of the American Board of Obstetrics and Gynecology regarding the care of men by gynecologists, but perhaps it is worth considering and acknowledging the policy.
Guidelines & “Consumerization-Driven” Cattle
The authors lamented that “guideline-nonconformant care has been driven by the consumerization of sexual health.” If they mean by “guideline-nonconformant care” that the care is not in compliance with the American Urological Association written in 2018, then perhaps the previous review of the literature would reassure the authors that the guidelines may need revision.
As for impotent men being “driven” like dumb cattle to the slaughter by “consumerization of sexual health,” perhaps, a more accurate view would be that smartmen are seeking help– motivated by the pain of broken relationships and loss of self-esteem, to find therapies that match the current research so that they can, if possible, avoid the risks and expense of PDE5Is and surgery (both risks & expense being more with PDE5Is than with a P-Shot® procedure).
A little more history about guidelines…
As another example of how guidelines can become out of date, a review article in Urology (Finkle1980) said, “most instances of acquired impotence are psychogenic. Any nonjudgmental, competent practitioner [urologist] can aid victims of psychogenic impotence by a ‘listening and encouragement’ method. Urologists, in particular, are commonly confronted with genital sexual problems and may be best suited as primary therapists by developing interest in urologic counseling.” In review, in 1980, 85% of ED was thought, by the Amerian Board of Urology, to be psychogenic; so, urologists were encouraged to learn to be sex therapists. Then, when an ineffective blood pressure pill accidentally turned out to be an effective ED pill because it improved blood flow, guidelines needed revision, and now instead of stating that 85% of ED is psychogenic, 85% of ED is thought to be neurovascular. So, perhaps, when employing 4-year-old guidelines, one might pause and consider the anguish experienced by a man back in the 1980s who suffered ED from neurovascular disease while being told that his inability to make love to his wife would go away if he would just put his thoughts in order through sex-therapy with his urologist.
Advertising: Noble or Evil?
The authors were concerned that “advertising is associated with patient demand, particularly in men’s health.” But is not advertising associated with the demand for almost everything? Is not that what advertising does? But, patient demand is also associated with the degree of suffering; and, the broken relationships and sexual dysfunction (for which men seek help with the P-Shot®) cause severe psychological and social distress. Also, the number of dollars spent advertising Viagra and male surgeries dwarfs that spent on advertising PRP treatments; because there is no drug to sell with a PRP treatment, one will likely never see an ad for PRP while watching pro sports; but, such ads are frequent for Viagra® and male surgeries. Still, though Viagra® is associated with hundreds of cases of blindness every year (even when used properly), and far more is spent on advertising for Viagra than is spent on PRP, such advertising of Viagra® is still legitimate as long as it is honest about what is possible and the risks involved. The layperson, moreover, cannot be expected to be up to date about the latest therapies; the best advertising educates the person suffering from disease about their disease process and about their possible methods of treatment; when deployed in this way, advertising is needed and noble so that suffering people may know how to find help.It is not the responsibility of the layperson to know what the physician is able to do for them; it is the responsibility of physicians to educate people about both diseases and possible treatments of diseases–that noble goal should be at the heart of all “advertising.”
Have you seen a picture of “These”?
The authors also worry that “these companies have been shown to omit appropriate medical evaluation, which may lead to patient harm.” (Shahinyan et al., 2022, p. 2 Comparing companies that dispensed medications without doing a physical exam with P-Shot® physicians who must physically (not remotely) see the patient to do a procedure does not seem logical. Also, the authors mention advertising platforms and include groups as diverse as gynecologists, chiropractors, and “unknown,” one might wonder how to recognize what “these” even means. We agree, however, with the authors about the need for standardization (as stated previously in this note) and, seeing the wide variety that happened with hyaluronic acid filler injections, tried to avoid these dangers by the standardization of protocols that are embedded in the P-Shot® procedure. Then we, the thousands of doctors who are members of the CMA, backed up that philosophy with a decade of teaching and millions in legal battles in 55 countries).
There is more in an “®” than meets the eye of some people.
What do PRP, Shock Wave, and Stem Cells Share?
The authors classify as “experimental” three types of treatments in their statement about “experimental ED therapies, such as PRP injections, low-intensity shockwave therapy, and autologous stem cell injections.”
Experimental by policy?
If what is meant by “experimental” is that which is not yet approved by a policy that was made 4 years ago and by this paper which seems unaware of the research of the past 4 years, then perhaps the definition of what is experimental needs revision/updating.
Experimental by FDA?
If what is meant by experimental is that which is not yet approved by the FDA, then the grouping of these three is misleading since stem cells are regulated by the FDA, but PRP is still considered simply the person’s own tissue, like hair, or skin, or urine; so, PRP is not regulated by the FDA. Procedures are also not regulated by the FDA at all (not prostatectomy or hysterectomy, no procedure, ever). But devices are regulated by the FDA and the Cellular Medicine Association recommends that the P-Shot® procedure be done only with centrifuges that have been cleared by the FDA for the preparation of PRP to go back into the body (which is a different level of clearance than preparing blood for laboratory analysis). Also, consider that there is still no FDA-approved form of testosterone for women. And testosterone for women when given by adjusting the dose of forms normally given to men is not often not covered by insurance. Also, the research supporting shock wave therapy for neovascularization is also very compelling and the therapy has been proven to be safe and effective.
Experimental by Insurance?
Perhaps, the authors meant by “experimental” that there is still no insurance coverage for either PRP or shock wave therapy and so patients must be either treated for free (at the considerable expense of time and money to the doctor) or the patients must be charged. This definition seems to personify the metaphor of the tail wagging the cow: should physicians really wait for the necessarily profit-driven insurance corporations to tell us what is good medicine? That seems to be a growing and pervasive attitude. There are many examples of the gap between the recognition of what is helpful and what is covered by insurance. For example, there is no insurance coverage for Nike® shoes, but walking (when sufficient in volume) has been determined to be better at preventing heart attack than any diabetes or hypertension drug on the market. Also, since PRP is the patient’s own blood and the device manufacturers cannot channel any cost of advertising to their particular device, there is little incentive by the device manufacturers and none by any pharmaceutical company to finance research to obtain the needed data to demand insurance coverage. The research sponsored by the CMA is minuscule compared to what is possible by the manufacturers of VIagra. As another example, a study by Ronald Virag (referenced previously) demonstrated that PRP worked better than Xyflex for Peyronie’s disease at considerably less cost, with no risk of penile fracture (compared to around 1 in 50 of those who receive Xyflex), no downtime wiht the PRP, and the side effect of ED function going up by an average of 7 on the shim score! But you do not see ads about PRP as you do for Xyflex, and you see few large-scale studies because the funding is just not there. And you do not see an insurance code to reimburse for the procedure.
Also, placebo-control studies of PRP are difficult because saline (often used as a placebo) has effects of its own and as a stand-alone therapy has been used to treat scarring and promote tissue growth. So, saline’s appropriateness as a placebo has been questioned when studies involve the injection of materials intended to regenerate tissue with a hydrodissection-like delivery.
Limitations, Corrections, and Conversations
The authors concede that the study does have one (and only one) limitation: “A limitation of this study is the selective focus on large metropolitan areas, which may not be representative of smaller or rural areas.” (Shahinyan et al., 2022, p. 3.
But, perhaps, the study has more than one limitation including at least all of the following:
Assuming that a policy made 4 years ago would reflect the most up do date thinking that should be applied in today’s clinic.
Assuming that everyone using PRP is operating without any standardization and ignoring the fact that those who are licensed by the Cellular Medicine Association to use the “P-Shot®” name have all studied the same protocol and agreed (with a signed document) to a specific standardization in regards to materials, methods, indications, pre-procedure & post-procedure protocols, and agree to refund all money when the patient is not satisfied with the results or the procedure.
Assuming that gynecologists are incapable of understanding men’s sexual dysfunction–ignoring the fact that the American College of Obstetrics and Gynecology (ACOG) has agreed that gynecologists are, in fact, as able to care for men as are urologists to care for women.
Assuming that those who are licensed to do the P-Shot® can be of any training, ignoring the fact the CMA only licenses the use of the service mark, Priapus Shot® (P-Shot®), to those whose license would also cover the use of hyaluronic acid injections in the state in which the provider practices; such medical license would still not qualify the provider to advertise the procedure, but would be required to able to undergo training to learn how to do the procedure.
Assuming a “paucity” of research to support the idea of PRP for the treatment of ED without acknowledging the noticeable and growing body of research supporting that idea (much of which appeared after the referenced opinion of the American College of Urologists).
Assuming that the degree of the advertising of PRP (directed toward men with ED) implies bad medicine when, in fact, much more is spent advertising PDE5Is for men with ED than is spent advertising PRP. More lifetime expense and a greater risk of serious sequelae (including blindness and stroke) are associated with PDE5Is than are associated with PRP (which has never caused either of these). In summary, the article erroneously ignores that the amount of advertising for a procedure in no way correlates with either the effectiveness of a procedure or its risks; instead, the article seems to imply the erroneous and opposite opinion that there is a correlation.
Overall, I am grateful to the authors for bringing attention to the P-Shot® and would invite them to read the current research and to consider helping further that research by joining the Cellular Medicine Association (CMA). The CMA has spent millions in doing exactly what the authors imply needs to be done: quality control, standardization, and further research. We (CMA members) grieve that the authors seem unaware of our existence or purpose. We have done hundreds of thousands of P-Shot® procedures over the past decade, but we need more help to do the needed research and to supply the demand for both the training of physicians and the provision of the service to men suffering from ED.
Future Research
First, comes an understanding of a new concept; then, after proof-of-concept, comes the study of the infinite variabilities that may affect the results and risks of the new concept: for example the following are only some of the questions that need answers regarding the use of PRP for ED:
Who is most likely to be helped by PRP injections into the corpus cavern and who is least likely to be helped?
How can the idea be integrated into penile rehabilitation post-prostatectomy?
What injection technique variations would work best for Peyronie’s disease, trauma (bicycle, surgery), diabetes, BXO.
Could PRP be used to improve the effectiveness of ED drugs, and to improve outcomes with penile implants (sensation and wound healing).
What can be done with the PRP to improve its effectiveness? For, example, studies have shown that washing the platelets or cooling the platelets, aerobic exercise just prior to phlebotomy, or fasting prior to phlebotomy can all have beneficial effects.
What patient factors would interfere with the effectiveness of the treatment? For example, some NSAIDS will attenuate the effectiveness and of course smoking (often left out of study inclusion and exclusion criterion), nutrition status, and platelet counts—all can have effects.
Can effects similar to PRP be seen for ED with whole blood or saline?
If saline has effects of its own when used to hydrodissect tissue, how should PRP studies be conducted? Is it possible to have a double-blind placebo-controlled study, or is PRP similar to birth-control pills, hysterectomy, and parachutes where perhaps the mechanics and ethics of double-blind placebo control studies make them impossible.
What Now?
The orthopedic surgeons and dentists have at least a decade-long head start in regards to how and when to use PRP; likely, much of their observations and conversations can be extrapolated to the sexual dysfunction, urology, and gynecology world. Suffering women and men need physicians to think deeply, and when the benefits outweigh the risks (and the monetary risk to the patient is made zero), informed patients and educated providers should be encouraged to proceed. I hope you’ll consider the following resources. Here’s where you can apply to learn to do the P-Shot® procedure. Here is where you can find a licensed P-Shot® provider.
References that inspired Runels to develop the P-Shot® procedure (describing the need for a better way and suggesting the use of blood-derived growth factors)
1. Siroky MB, Azadzoi KM. Vasculogenic Erectile Dysfunction: Newer Therapeutic Strategies. Journal of Urology. 2003;170(2S):S24-S30. doi:10.1097/01.ju.0000075361.35942.17
2.
Garcia M, Fandel T, Lin G, et al. Treatment of erectile dysfunction in the obese type 2 diabetic ZDF rat with adipose tissue-derived stem cells. Published online 2010:14.
Reference from Sclafani that also prompted the P-Shot® procedure development
Sclafani AP, McCormick SA. Induction of dermal collagenesis, angiogenesis, and adipogenesis in human skin by injection of platelet-rich fibrin matrix. Arch Facial Plast Surg. 2012;14(2):132-136. doi:10.1001/archfacial.2011.784
Review of the Thrombin Cascade and It’s Relation to PRP
Smith SA, Travers RJ, Morrissey JH. How it all starts: Initiation of the clotting cascade. Critical Reviews in Biochemistry and Molecular Biology. 2015;50(4):326-336. doi:10.3109/10409238.2015.1050550
Finkle AL. Sexual impotency: Current knowledge and treatment I. Urology/sexuality clinic. Urology. 1980;16(5):449-452. doi:10.1016/0090-4295(80)90592-0
References about treating acne scars with PRP
1.
Bhargava S, Goldust M, Singer H, Negbenebor N, Kroumpouzos G. Evaluating resurfacing modalities in aesthetics. Clin Dermatol. 2022;40(3):274-282. doi:10.1016/j.clindermatol.2021.01.019
2.
Majid I, Timungpi R. Platelet rich Plasma (PRP) in treatment of Topical steroid damaged face (TSDF): a retrospective analytical study. Dermatologic Therapy. n/a(n/a). doi:10.1111/dth.15356
3.
Peng GL. Platelet-Rich Plasma for Skin Rejuvenation: Facts, Fiction, and Pearls for Practice. Facial Plastic Surgery Clinics of North America. Published online 2019. doi:10.1016/j.fsc.2019.04.006
4.
Cui X, Ma Y, Wang H, Huang J, Li L, Cheng B. The Anti-photoaging Effects of Pre- and Post-treatment of Platelet-rich Plasma on UVB-damaged HaCaT Keratinocytes. :38.
5.
Alser OH, Goutos I. The evidence behind the use of platelet-rich plasma (PRP) in scar management: a literature review. Scars, Burns & Healing. 2018;4:205951311880877. doi:10.1177/2059513118808773
References about the other indications regarding PRP
References about improving hair
1.
Gupta AK, Bamimore MA. The effect of placebo in split-scalp and whole-head platelet-rich plasma trials for androgenetic alopecia differs: Findings from a systematic review with quantitative evidence syntheses. J Cosmet Dermatol. Published online January 31, 2022. doi:10.1111/jocd.14813
2.
Berebichez-Fridman R, Montero-Olvera PR. Sources and Clinical Applications of Mesenchymal Stem Cells: State-of-the-art review. Sultan Qaboos University Medical Journal [SQUMJ]. 2018;18(3):e264-277. doi:10.18295/squmj.2018.18.03.002
3.
Ozcan KN, Sener S, Altunisik N, Turkmen D. PRP application by dermapen microneedling and intradermal point-by-point injection methods, and their comparison with clinical findings and trichoscan in patients with androgenetic alopecia. Dermatologic Therapy. n/a(n/a). doi:10.1111/dth.15182
4.
Jha AK, Vinay K, Zeeshan M, Roy PK, Chaudhary RKP, Priya A. Platelet-rich Jha, A. K., Vinay, K., Zeeshan, M., Roy, P. K., Chaudhary, R. K. P., & Priya, A. (2019). Platelet-rich plasma and microneedling improves hair growth in patients ofandrogenetic alopecia when used as an adjuvant to minoxidil. Journal of Cosmet. Journal of Cosmetic Dermatology. Published online 2019. doi:10.1111/jocd.12864
Anudeep TC, Jeyaraman M, Muthu S, et al. Advancing Regenerative Cellular Therapies in Non-Scarring Alopecia. Pharmaceutics. 2022;14(3):612. doi:10.3390/pharmaceutics14030612
7.
Anudeep TC, Jeyaraman M, Muthu S, et al. Advancing Regenerative Cellular Therapies in Non-Scarring Alopecia. Pharmaceutics. 2022;14(3):612. doi:10.3390/pharmaceutics14030612
8.
Wall D, Meah N, Fagan N, York K, Sinclair R. Advances in hair growth. Fac Rev. 2022;11:1. doi:10.12703/r/11-1
References about helping with female urinary incontinence
1.
Kirchin V, Page T, Keegan PE, et al. Urethral injection therapy for urinary incontinence in women. The Cochrane Database of Systematic Reviews. 2017;2017(7). doi:10.1002/14651858.CD003881.pub4
2.
Athanasiou S, Kalantzis C, Zacharakis D, Kathopoulis N, Pontikaki A, Grigoriadis T. The Use of Platelet-rich Plasma as a Novel Nonsurgical Treatment of the Female Stress Urinary Incontinence: A Prospective Pilot Study. Female Pelvic Med Reconstr Surg. 2021;27(11):e668-e672. doi:10.1097/SPV.0000000000001100
3.
Samy Tahoon A, El-Din Hussein Salem H, Anwar Abdo Mousa A. The Role of Platelet Rich Plasma Injections in Cases of Stress Incontinence.; 2022. doi:10.32388/KG77ZQ
4.
Joseph C, Srivastava K, Ochuba O, et al. Stress Urinary Incontinence Among Young Nulliparous Female Athletes. Cureus. 2021;13(9). doi:10.7759/cureus.17986
5.
Zhou S, Zhang K, Atala A, et al. Stem Cell Therapy for Treatment of Stress Urinary Incontinence: The Current Status and Challenges. doi:10.1155/2016/7060975
6.
Nikolopoulos KI, Pergialiotis V, Perrea D, Doumouchtsis SK. Restoration of the pubourethral ligament with platelet rich plasma for the treatment of stress urinary incontinence. Medical Hypotheses. 2016;90:29-31. doi:10.1016/j.mehy.2016.02.019
7.
PANDIT M, DELANCEY JOL, ASHTON-MILLER JA, IYENGAR J, BLAIVAS M, PERUCCHINI D. Quantification of Intramuscular Nerves Within the Female Striated Urogenital Sphincter Muscle. Obstet Gynecol. 2000;95(6 Pt 1):797-800. Accessed October 20, 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1192577/
8.
Gorton E, Stanton S, Monga A, Wiskind AK, Lentz GM, Bland DR. Periurethral collagen injection: a long-term follow-up study. BJU international. 1999;84(9):966-971. Accessed August 24, 2015. http://www.ncbi.nlm.nih.gov/pubmed/10571621
9.
Lee PE, Kung RC, Drutz HP. PERIURETHRAL AUTOLOGOUS FAT INJECTION AS TREATMENT FOR FEMALE STRESS URINARY INCONTINENCE: A RANDOMIZED DOUBLE-BLIND CONTROLLED TRIAL. Journal of Urology. 2001;165(1):153-158. doi:10.1097/00005392-200101000-00037
10.
Ford AA, Rogerson L, Cody JD, Ogah J. Mid‐urethral sling operations for stress urinary incontinence in women. Cochrane Database of Systematic Reviews. 2015;(7). doi:10.1002/14651858.CD006375.pub3
11.
Zubieta M, Carr RL, Drake MJ, Bø K. Influence of voluntary pelvic floor muscle contraction and pelvic floor muscle training on urethral closure pressures: a systematic literature review. Int Urogynecol J. 2016;27(5):687-696. doi:10.1007/s00192-015-2856-9
12.
O’Connor E, Riogh AN an, Karavitakis M, Monagas S, Nambiar A. Diagnosis and Non-Surgical Management of Urinary Incontinence – A Literature Review with Recommendations for Practice. IJGM. 2021;14:4555-4565. doi:10.2147/IJGM.S289314
Oshiro T, Kimura R, Izumi K, Ashikari A, Saito S, Miyazato M. Changes in urethral smooth muscle and external urethral sphincter function with age in rats. Physiological Reports. 2021;8(24):e14643. doi:10.14814/phy2.14643
15.
Callewaert G, Da Cunha MMCM, Sindhwani N, Sampaolesi M, Albersen M, Deprest J. Cell-based secondary prevention of childbirth-induced pelvic floor trauma. Nat Rev Urol. 2017;14(6):373-385. doi:10.1038/nrurol.2017.42
16.
Perucchini D, DeLancey JOL, Ashton-Miller JA, Galecki A, Schaer GN. Age effects on urethral striated muscle II. Anatomic location of muscle loss. American Journal of Obstetrics and Gynecology. 2002;186(3):356-360. doi:10.1067/mob.2002.121090
17.
Perucchini D, DeLancey JO, Ashton-Miller JA, Peschers U, Kataria T. Age effects on urethral striated muscle I. changes in number and diameter of striated muscle fibers in the ventral urethra. American Journal of Obstetrics & Gynecology. 2002;186(3):351-355. doi:10.1067/mob.2002.121089
18.
Wiśniewska-Ślepaczuk K, Pieczykolan A, Grzesik-Gąsior J, Wdowiak A. A Review of Aesthetic Gynecologic Procedures for Women. Plastic Surgical Nursing. 2021;41(4):191-202. doi:10.1097/PSN.0000000000000400
19.
Long CY, Lin KL, Shen CR, et al. A pilot study: effectiveness of local injection of autologous platelet-rich plasma in treating women with stress urinary incontinence. Sci Rep. 2021;11(1):1584. doi:10.1038/s41598-020-80598-2
References regarding the use of PRP to help with female orgasm
1.
Handy AB, Stanton AM, Meston CM. Understanding Women’s Subjective Sexual Arousal Within the Laboratory: Definition, Measurement, and Manipulation. Sexual Medicine Reviews. 2018;6(2):201-216. doi:10.1016/j.sxmr.2017.11.001
2.
Sanoulis V, Nikolettos N, Vlahos N. The use of Platelet-Rich Plasma in the Gynaecological Clinical Setting. A review. 2019;18(3):11.
3.
Prodromidou A, Zacharakis D, Athanasiou S, et al. The Emerging Role on the Use of Platelet-Rich Plasma Products in the Management of Urogynaecological Disorders. Surg Innov. Published online April 28, 2021:15533506211014848. doi:10.1177/15533506211014848
4.
Matz EL, Pearlman AM, Terlecki RP. Safety and feasibility of platelet rich fibrin matrix injections for treatment of common urologic conditions. Investig Clin Urol. 2018;59(1):61-65. doi:10.4111/icu.2018.59.1.61
5.
Jb N. O-Shot: Platelets Rich Plasma in Intimate Female Treatment. Published online 2017:4.
6.
Sharp G, Maynard P, Hamori CA, Oates J, Sarwer DB, Kulkarni J. Measuring Quality of Life in Female Genital Cosmetic Procedure Patients: A Systematic Review of Patient-Reported Outcome Measures. Aesthetic Surgery Journal. 2020;40(3):311-318. doi:10.1093/asj/sjz325
7.
Zheng Z. Materials Selection for the Injection into Vaginal Wall for Treatment of Vaginal Atrophy. Published online 2021:11.
8.
Hersant B, SidAhmed-Mezi M, Belkacemi Y, et al. Efficacy of injecting platelet concentrate combined with hyaluronic acid for the treatment of vulvovaginal atrophy in postmenopausal women with history of breast cancer. Menopause. 2018;25(10):1. doi:10.1097/GME.0000000000001122
9.
Long CY. A pilot study: effectiveness of local injection of autologous platelet-rich plasma in treating women with stress urinary incontinence. Scientific Reports. Published online 2021:9.
10.
Runels C. A Pilot Study of the Effect of Localized Injections of Autologous Platelet Rich Plasma (PRP) for the Treatment of Female Sexual Dysfunction. J Women’s Health Care. 2014;03(04). doi:10.4172/2167-0420.1000169
References Regarding the treatment of Interstitial cystitis with PRP
1.
Trama F, Illiano E, Marchesi A, et al. Use of Intravesical Injections of Platelet-Rich Plasma for the Treatment of Bladder Pain Syndrome: A Comprehensive Literature Review. Antibiotics (Basel). 2021;10(10):1194. doi:10.3390/antibiotics10101194
2.
Ke QS, Jhang JF, Lin TY, et al. Therapeutic potential of intravesical injections of platelet-rich plasma in the treatment of lower urinary tract disorders due to regenerative deficiency. Ci Ji Yi Xue Za Zhi. 2019;31(3):135-143. doi:10.4103/tcmj.tcmj_92_19
3.
Mirzaei M, Daneshpajooh A, Farsinezhad A, et al. The Therapeutic Effect of Intravesical Instillation of Platelet Rich Plasma on Recurrent Bacterial Cystitis in Women: A Randomized Clinical Trial. Urol J. 2019;16(6):609-613. doi:10.22037/uj.v0i0.5239
4.
Dönmez Mİ, İnci K, Zeybek ND, Doğan HS, Ergen A. The Early Histological Effects of Intravesical Instillation of Platelet-Rich Plasma in Cystitis Models. Int Neurourol J. 2016;20(3):188-196. doi:10.5213/inj.1632548.274
5.
Huang YC, Chuang YC. Reply to the Commentary on “New Frontiers or the Treatment of Interstitial Cystitis/Bladder Pain Syndrome-Focused on Stem Cells, Platelet-Rich Plasma, and Low-Energy Shock Wave.” Int Neurourol J. 2020;24(4):389-390. doi:10.5213/inj.2040414.207
6.
Jiang YH, Kuo YC, Jhang JF, et al. Repeated intravesical injections of platelet-rich plasma improve symptoms and alter urinary functional proteins in patients with refractory interstitial cystitis. Sci Rep. 2020;10(1):15218. doi:10.1038/s41598-020-72292-0
7.
Jhang JF, Wu SY, Lin TY, Kuo HC. Repeated intravesical injections of platelet-rich plasma are effective in the treatment of interstitial cystitis: a case control pilot study. Low Urin Tract Symptoms. 2019;11(2):O42-O47. doi:10.1111/luts.12212
8.
Ozyuvali E, Yildirim ME, Yaman T, Kosem B, Atli O, Cimentepe E. Protective Effect of Intravesical Platelet-Rich Plasma on Cyclophosphamide-Induced Hemorrhagic Cystitis. Clin Invest Med. 2016;39(6):27514.
9.
Chen YH, Man KM, Chen WC, et al. Platelet-Rich Plasma Ameliorates Cyclophosphamide-Induced Acute Interstitial Cystitis/Painful Bladder Syndrome in a Rat Model. Diagnostics (Basel). 2020;10(6):E381. doi:10.3390/diagnostics10060381
10.
Jhang JF, Lin TY, Kuo HC. Intravesical injections of platelet-rich plasma is effective and safe in treatment of interstitial cystitis refractory to conventional treatment-A prospective clinical trial. Neurourology and Urodynamics. 2018;(October). doi:10.1002/nau.23898
11.
Jhang JF, Jiang YH, Hsu YH, et al. Improved Urothelial Cell Proliferation, Cytoskeleton and Barrier Function Protein Expression in the Patients With Interstitial Cystitis/Bladder Pain Syndrome After Intravesical Platelet-Rich Plasma Injection. Int Neurourol J. 2022;26(Suppl 1):S57-67. doi:10.5213/inj.2142100.050
12.
Riccetto CLZ. Editorial Comment: Intravesical injections of platelet-rich plasma is effective and safe in treatment of interstitial cystitis refractory to conventional treatment-A prospective clinical trial. Int Braz J Urol. 2021;47(2):456-457. doi:10.1590/S1677-5538.IBJU.2021.02.04
References regarding the treatment of mesh complications in women with PRP
1.
Prodromidou A, Zacharakis D, Athanasiou S, et al. The Emerging Role on the Use of Platelet-Rich Plasma Products in the Management of Urogynaecological Disorders. Surg Innov. Published online April 28, 2021:15533506211014848. doi:10.1177/15533506211014848
2.
Di Nicola V, Tebala GD. Platelet-Rich Fibrin-Mesh Technique for Inguinal Hernia Repair: Results of a Feasibility Pilot Study. Surg Technol Int. 2021;38:175-177.
3.
Lorenz J, Al-Maawi S, Sader R, Ghanaati S. Individualized Titanium Mesh Combined With Platelet-Rich Fibrin and Deproteinized Bovine Bone: A New Approach for Challenging Augmentation. Journal of Oral Implantology. 2018;44(5):345-351. doi:10.1563/aaid-joi-D-18-00049
4.
Belebecha V, Casagrande R, Urbano MR, et al. Effect of the platelet-rich plasma covering of polypropylene mesh on oxidative stress, inflammation, and adhesions. Int Urogynecol J. 2020;31(1):139-147. doi:10.1007/s00192-019-03938-5
5.
Parizzi NG, Rubini OÁ, Almeida SHM de, Ireno LC, Tashiro RM, Carvalho VHT de. Effect of platelet-rich plasma on polypropylene meshes implanted in the rabbit vagina: histological analysis. International braz j urol : official journal of the Brazilian Society of Urology. 43(4):746-752. doi:10.1590/S1677-5538.IBJU.2016.0177
6.
Medel S, Alarab M, Kufaishi H, Drutz H, Shynlova O. Attachment of Primary Vaginal Fibroblasts to Absorbable and Nonabsorbable Implant Materials Coated With Platelet-Rich Plasma: Potential Application in Pelvic Organ Prolapse Surgery. Female Pelvic Medicine & Reconstructive Surgery. 2015;21(4):190-197. doi:10.1097/SPV.0000000000000178
7.
Castellani D, Valloni A, Piccirilli A, Paradiso Galatioto G, Vicentini C. An innovative approach to treating vaginal mesh exposure after abdominal sacral colpopexy: endoscopic resection of mesh and platelet-rich plasma; initial experience in three women. Int Urogynecol J. 2017;28(2):325-327. doi:10.1007/s00192-016-3154-x
References Supporting PRP For ED and Peyronie’s Disease
1.
Siroky MB, Azadzoi KM. Vasculogenic Erectile Dysfunction: Newer Therapeutic Strategies. Journal of Urology. 2003;170(2S). doi:10.1097/01.ju.0000075361.35942.17
2.
Garcia M, Fandel T, Lin G, et al. Treatment of erectile dysfunction in the obese type 2 diabetic ZDF rat with adipose tissue-derived stem cells. Published online 2010:14.
3.
Towe M, Peta A, Saltzman RG, Balaji N, Chu K, Ramasamy R. The use of combination regenerative therapies for erectile dysfunction: rationale and current status. Int J Impot Res. Published online July 12, 2021:1-4. doi:10.1038/s41443-021-00456-1
4.
Raheem AA, Garaffa G, Raheem TA, et al. The role of vacuum pump therapy to mechanically straighten the penis in Peyronie’s disease. BJU International. 2010;106(8):1178-1180. doi:10.1111/j.1464-410X.2010.09365.x
5.
Israeli JM, Lokeshwar SD, Efimenko IV, Masterson TA, Ramasamy R. The potential of platelet-rich plasma injections and stem cell therapy for penile rejuvenation. Int J Impot Res. Published online November 6, 2021:1-8. doi:10.1038/s41443-021-00482-z
6.
Matz EL, Pearlman AM, Terlecki RP. Safety and feasibility of platelet rich fibrin matrix injections for treatment of common urologic conditions. Investig Clin Urol. 2018;59(1):61-65. doi:10.4111/icu.2018.59.1.61
7.
Liu MC, Chang ML, Wang YC, Chen WH, Wu CC, Yeh SD. Revisiting the Regenerative Therapeutic Advances Towards Erectile Dysfunction. Cells. 2020;9(5):1250. doi:10.3390/cells9051250
8.
Everts P, Onishi K, Jayaram P, Lana JF, Mautner K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int J Mol Sci. 2020;21(20):7794. doi:10.3390/ijms21207794
9.
Matz EL, Scarberry K, Terlecki R. Platelet-Rich Plasma and Cellular Therapies for Sexual Medicine and Beyond. Sexual Medicine Reviews. 2022;10(1):174-179. doi:10.1016/j.sxmr.2020.07.001
10.
Poulios E, Mykoniatis I, Pyrgidis N, et al. Platelet-Rich Plasma (PRP) Improves Erectile Function: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial. Journal of Sexual Medicine. 2021;18(5):926-935. doi:10.1016/j.jsxm.2021.03.008
11.
Schirmann A, Boutin E, Faix A, Yiou R. Pilot study of intra-cavernous injections of platelet-rich plasma (P-shot®) in the treatment of vascular erectile dysfunction. Progrès en Urologie. Published online June 2022:S1166708722001300. doi:10.1016/j.purol.2022.05.002
12.
Chung E. medical sciences A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Published online 2019:1-11.
13.
Pruimboom L, Muskiet FAJ. Intermittent living; the use of ancient challenges as a vaccine against the deleterious effects of modern life – A hypothesis. Medical Hypotheses. 2018;120:28-42. doi:10.1016/J.MEHY.2018.08.002
14.
Calabrese EJ. Hormesis: Why it is important to toxicology and toxicologists. Environmental Toxicology and Chemistry. 2008;27(7):1451-1474. doi:10.1897/07-541.1
15.
Ruffo A, Franco M, Illiano E, Stanojevic N. Effectiveness and safety of Platelet rich Plasma (PrP) cavernosal injections plus external shock wave treatment for penile erectile dysfunction: First results from a prospective, randomized, controlled, interventional study. European Urology Supplements. 2019;18(1):e1622-e1623. doi:10.1016/S1569-9056(19)31175-3
16.
Bosma-Den Boer MM, Van Wetten ML, Pruimboom L. Chronic inflammatory diseases are stimulated by current lifestyle: How diet, stress levels and medication prevent our body from recovering. Nutrition and Metabolism. 2012;9. doi:10.1186/1743-7075-9-32
17.
Casabona F, Gambelli I, Casabona F, Santi P, Santori G, Baldelli I. Autologous platelet-rich plasma (PRP) in chronic penile lichen sclerosus: the impact on tissue repair and patient quality of life. Int Urol Nephrol. 2017;49(4):573-580. doi:10.1007/s11255-017-1523-0
18.
Chung. A Review of Current and Emerging Therapeutic Options for Erectile Dysfunction. Medical Sciences. 2019;7(9):91. doi:10.3390/medsci7090091
19.
Lee PJ, Jiang YH, Kuo HC. A novel management for postprostatectomy urinary incontinence: platelet-rich plasma urethral sphincter injection. Scientific Reports |. 123AD;11:5371. doi:10.1038/s41598-021-84923-1
20.
Littara A, Palmieri B, Rottigni V, Iannitti T. A clinical study to assess the effectiveness of a hyaluronic acid-based procedure for treatment of premature ejaculation. International Journal of Impotence Research. 2013;25(3). doi:10.1038/ijir.2013.13
21.
Kumar CS. 265 Combined Treatment of Injecting Platelet Rich Plasma With Vacuum Pump for Penile Enlargement. The Journal of Sexual Medicine. 2017;14(1):S78. doi:10.1016/j.jsxm.2016.11.174
References regarding the use of PRP to help with infertility in women
1.
Merhi Z, Seckin S, Mouanness M. REPRODUCTIVE ENDOCRINOLOGY: CASE STUDY Intraovarian PRP Injection Improved Hot Flashes in a Woman With Very Low Ovarian Reserve. doi:10.1007/s43032-021-00655-7
2.
Sills ES, Li X, Rickers NS, Wood SH, Palermo GD. Metabolic and neurobehavioral response following intraovarian administration of autologous activated platelet rich plasma: First qualitative data. Neuro endocrinology letters. 2019;39(6):427-433. Accessed October 31, 2019. http://www.ncbi.nlm.nih.gov/pubmed/30796792
References regarding the dangers of hyaluronic acid filler injection
References Showing that Saline Injected in a Study of Tissue Repair is Not a Placebo
1.
Saltzman BM, Leroux T, Meyer MA, et al. The Therapeutic Effect of Intra-articular Normal Saline Injections for Knee Osteoarthritis: A Meta-analysis of Evidence Level 1 Studies. Am J Sports Med. 2017;45(11):2647-2653. doi:10.1177/0363546516680607
2.
El-Amawy HS, Sarsik SM. Saline in Dermatology: A literature review. Journal of Cosmetic Dermatology. 2021;20(7):2040-2051. doi:10.1111/jocd.13813
3.
Searle T, Al-Niaimi F, Ali FR. Saline in dermatologic surgery. Journal of Cosmetic Dermatology. 2021;20(4):1346-1347. doi:10.1111/jocd.13996
4.
Bagherani N, R Smoller B. Introduction of a novel therapeutic option for atrophic acne scars: saline injection therapy. Glob Dermatol. 2016;2(6). doi:10.15761/GOD.1000159
5.
Asghar A, Tahir Z, Ghias A, Iftikhar U, Ahmad TJ. Efficacy and Safety of Intralesional Normal Saline in Atrophic Acne Scars. Annals of King Edward Medical University. 2019;25(2). doi:10.21649/akemu.v25i2.2867
6.
Sharma R, Gupta M, Rani R. Delineating injectable triamcinolone-induced cutaneous atrophy and therapeutic options in 24 patients—A retrospective study. Indian Dermatol Online J. 2022;13(2):199. doi:10.4103/idoj.idoj_483_21
7.
Clinical benefit of intra-articular saline as a comparator in clinical trials of knee osteoarthritis treatments_ A systematic review and meta-analysis of randomized trials | Elsevier Enhanced Reader. doi:10.1016/j.semarthrit.2016.04.003
Bokey EL, Keating JP, Zelas P. HYDRODISSECTION: AN EASY WAY TO DISSECT ANATOMICAL PLANES AND COMPLEX ADHESIONS. ANZ J Surg. 1997;67(9):643-644. doi:10.1111/j.1445-2197.1997.tb04616.x
10.
Popp LW. Improvement in Endoscopic Hernioplasty: Transcutaneous Aquadissection of the Musculofascial Defect and Preperitoneal Endoscopic Patch Repair. Journal of Laparoendoscopic Surgery. 1991;1(2):83-90. doi:10.1089/lps.1991.1.83
References regarding shock wave therapy for ED
1.
Low-Intensity Shockwave Therapy Improves Hemodynamic Parameters in Patients With Vasculogenic Erectile Dysfunction: A Triplex Ultrasonography-Based Sham-Controlled Trial.
2.
Kalyvianakis D, Hatzichristou D. Low-Intensity Shockwave Therapy Improves Hemodynamic Parameters in Patients With Vasculogenic Erectile Dysfunction: A Triplex Ultrasonography-Based Sham-Controlled Trial. The Journal of Sexual Medicine. 2017;14(7):891-897. doi:10.1016/j.jsxm.2017.05.012
3.
Yuan P, Ma D, Zhang Y, et al. Efficacy of low‐intensity extracorporeal shock wave therapy for the treatment of chronic prostatitis/chronic pelvic pain syndrome: A systematic review and meta‐analysis. Neurourology and Urodynamics. 2019;38(6):1457-1466. doi:10.1002/nau.24017
4.
Yuan P, Ma D, Zhang Y, et al. Efficacy of low-intensity extracorporeal shock wave therapy for the treatment of chronic prostatitis/chronic pelvic pain syndrome: A systematic review and meta-analysis. Neurourology and Urodynamics. 2019;38(6):1457-1466. doi:10.1002/nau.24017
Reference showing that Viagra works no better than placebo after prostate surgery
References showing the usefulness of PRP in downregulation of the auto-immune system (supportive of using PRP for the treatment of Peyronie’s disease)
1.
Behnia-Willison F, Pour NR, Mohamadi B, et al. Use of Platelet-rich Plasma for Vulvovaginal Autoimmune Conditions Like Lichen Sclerosus. Plast Reconstr Surg Glob Open. 2016;4(11):e1124. doi:10.1097/GOX.0000000000001124
2.
Borhani-Haghighi M, Mohamadi Y. The therapeutic effect of platelet-rich plasma on the experimental autoimmune encephalomyelitis mice. J Neuroimmunol. 2019;333:476958. doi:10.1016/j.jneuroim.2019.04.018
3.
Pototschnig H, Madl MT. Successful Treatment of Alopecia Areata Barbae with Platelet-rich Plasma. Cureus. 2020;12(4):e7495. doi:10.7759/cureus.7495
4.
Seffer I, Nemeth Z. Recovery from Bell Palsy after Transplantation of Peripheral Blood Mononuclear Cells and Platelet-Rich Plasma: Plastic and Reconstructive Surgery – Global Open. 2017;5(6):e1376. doi:10.1097/GOX.0000000000001376
5.
Tong S, Zhang C, Liu J. Platelet-rich plasma exhibits beneficial effects for rheumatoid arthritis mice by suppressing inflammatory factors. Mol Med Rep. 2017;16(4):4082-4088. doi:10.3892/mmr.2017.7091
6.
Rekik M, Mseddi M, Nadine K, Sellami K, Turki H. Efficacy of autologous platelet-rich plasma in the treatment of vitiligo : A 10- patient prospective study. Journal of Cosmetic Dermatology. n/a(n/a). doi:10.1111/jocd.15050
7.
Huber SC, de Lima Montalvão SA, Sachetto Z, Santos Duarte Lana JF, Annichino-Bizzacchi JM. Characterization of autologous platelet rich plasma (PRP) and its biological effects in patients with Behçet’s Disease. Regen Ther. 2021;18:339-346. doi:10.1016/j.reth.2021.08.010
8.
Anitua E, Pino A, Aspe L, et al. Anti-inflammatory effect of different PRGF formulations on cutaneous surface. Journal of Tissue Viability. 2021;30(2):183-189. doi:10.1016/j.jtv.2021.02.011
9.
Vazquez OA, Safeek RH, Komberg J, Becker H. Alopecia Areata Treated with Advanced Platelet-rich Fibrin Using Micronization. Plast Reconstr Surg Glob Open. 2022;10(1):e4032. doi:10.1097/GOX.0000000000004032
Sopko NA, Burnett AL. Erection rehabilitation following prostatectomy –current strategies and future directions. Nat Rev Urol. 2016;13(4):216-225. http://dx.doi.org/10.1038/nrurol.2016.47
Chung E. A review of regenerative therapies as penile rehabilitation in men following primary prostate cancer treatment: Evidence for erectile restoration and cavernous nerve regeneration. Asian Journal of Urology. 2022;9(3):287-293. doi:10.1016/j.ajur.2021.11.005
Lee PJ, Jiang YH, Kuo HC. A novel management for postprostatectomy urinary incontinence: platelet-rich plasma urethral sphincter injection. Scientific Reports |. 123AD;11:5371. doi:10.1038/s41598-021-84923-1
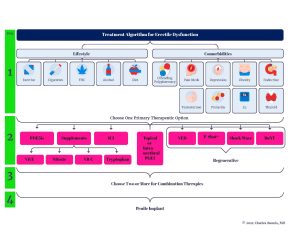
















 Stating that testosterone replacement for men grew in popularity solely as a health fad without mentioning the simultaneous explosion of research supporting the ways testosterone replacement may benefit an andropausal man could be discussed at length; but, since that would require a textbook, I will forgo that discussion and simply notice that
Stating that testosterone replacement for men grew in popularity solely as a health fad without mentioning the simultaneous explosion of research supporting the ways testosterone replacement may benefit an andropausal man could be discussed at length; but, since that would require a textbook, I will forgo that discussion and simply notice that 




 F
F








